Female Hair Loss in India: The Iron Deficiency, PCOS & Thyroid Connection
Female Hair Loss in India:
The Iron Deficiency, PCOS & Thyroid Connection
Why 50-60% of Indian women lose hair faster than Western counterparts-and what actually works beyond supplements and oils
Why Indian Women Experience Hair Loss at Unprecedented Rates
You've tried everything. Biotin supplements that promised thicker hair. Onion juice treatments your mother swears by. The expensive hair growth serum from that influencer. Six different dermatologists, each prescribing various medications and telling you to "reduce stress." Yet your ponytail is half the thickness it was three years ago, and the bathroom drain tells a story you're tired of reading every morning.
Here's what they didn't tell you: 50-60% of premenopausal Indian women have iron deficiency-the highest rate globally. Add to this a 10-15% PCOS* prevalence in urban areas, thyroid dysfunction affecting another 10% of women, predominantly vegetarian diets with poor protein absorption, and chronic stress levels that would make a Silicon Valley startup founder blush. You're not dealing with simple "hair fall." You're facing a perfect metabolic storm.
This is not a blog about miracle cures or grandmother's recipes. This is about understanding why Indian women lose hair at rates that shock international researchers, and which evidence-based treatments actually work when your ferritin levels are 12 ng/mL, your testosterone is elevated from PCOS, and your thyroid is quietly sabotaging every hair follicle on your scalp.
* PCOS (Polycystic Ovary Syndrome) is being renamed as Polyendocrine Metabolic Ovarian Syndrome (PMOS)
India's Iron Deficiency Crisis
Indian premenopausal women have the world's highest iron deficiency rate-compared to 10-15% in Western countries. This alone explains why "normal" hair loss treatments often fail in Indian patients.
The problem: Ferritin (stored iron) needs to be above 70 ng/mL for optimal hair growth. Most Indian women with hair loss have levels below 20 ng/mL. Lab reports may say "normal" (>15 ng/mL), but hair follicles disagree.
Iron Deficiency:
The Silent Epidemic Behind Diffuse Hair Loss
Why Iron Matters More Than You Think
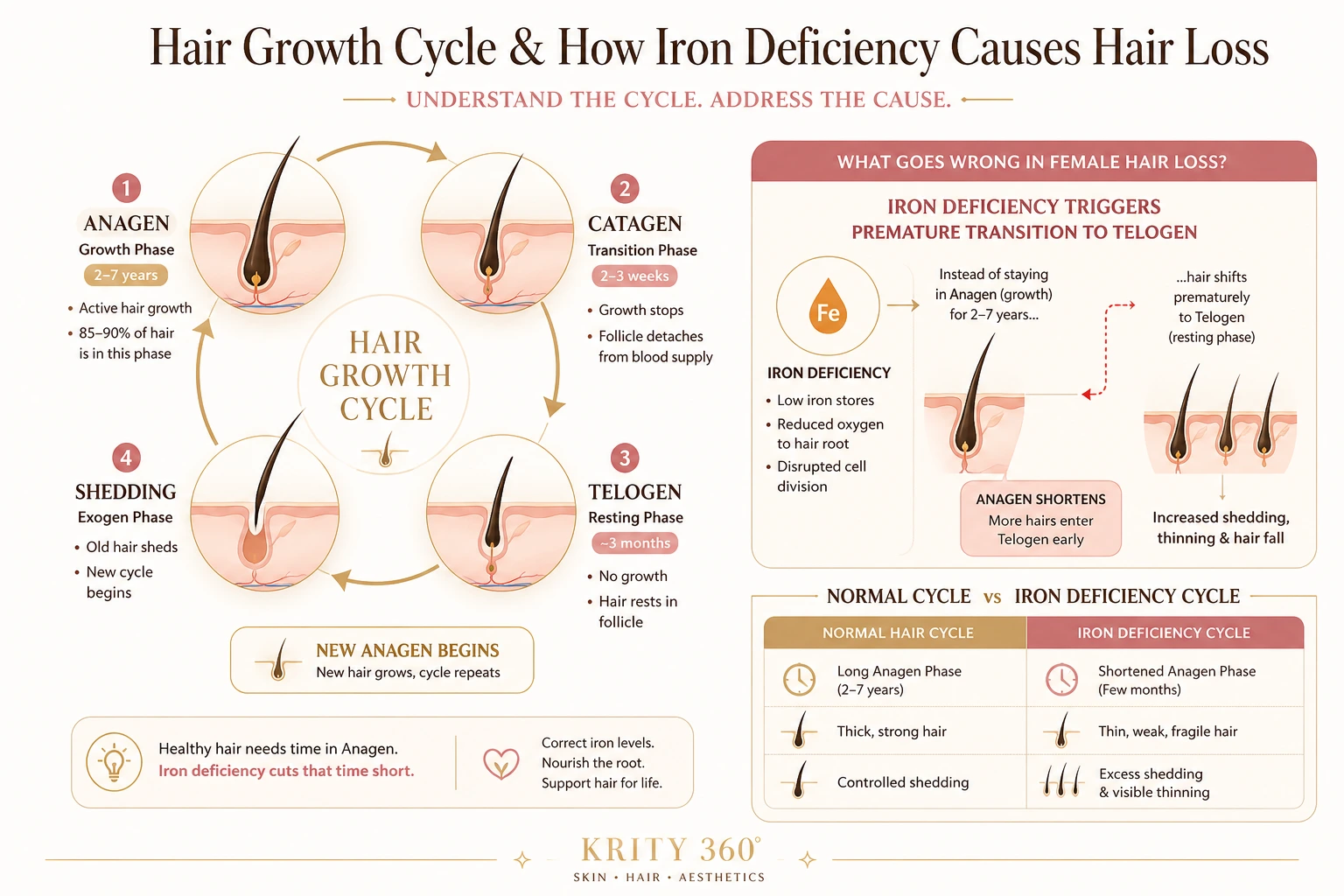
Hair follicles are metabolically hyperactive. They're among the fastest-dividing cells in your body, second only to bone marrow. This rapid cell division requires enormous amounts of iron to produce hemoglobin and ferritin-proteins essential for oxygen delivery and energy production.
When iron stores drop, your body implements triage: critical organs get first access to available iron, while "non-essential" tissues like hair follicles are starved. The result is telogen effluvium-excessive shedding that can persist for months even after iron levels normalize.
The Ferritin Threshold That Doctors Miss
Standard lab ranges define iron deficiency as ferritin below 15 ng/mL. But hair researchers have identified a different threshold: ferritin below 40 ng/mL causes hair loss, and optimal hair growth requires levels above 70 ng/mL.
This is why your doctor says "your iron is normal" while your hair continues thinning. Technically, you're not anemic. But your hair follicles are starving.
Why Indian Women Have the World's Highest Iron Deficiency Rates
1. Vegetarian Diet Dominance: Plant-based iron (non-heme iron) has 2-20% absorption compared to 15-35% for animal-based (heme) iron. Phytates in lentils, grains, and tea further block absorption. A vegetarian thali may contain adequate iron on paper, but your gut absorbs only a fraction.
2. Menstrual Blood Loss: Indian women lose 30-40 mL of blood per cycle on average. With heavy periods (common in PCOS and thyroid disorders), this increases to 60-80 mL. Each milliliter contains 0.5 mg of iron-chronic depletion that supplementation struggles to match.
3. Multiple Pregnancies and Breastfeeding: Each pregnancy depletes iron stores by 500-1000 mg. Breastfeeding requires 0.5-1 mg additional iron daily. Without aggressive supplementation between pregnancies, women enter a deficit cycle that worsens with each child.
4. Poor Gut Absorption: H. pylori infection (affecting 60-70% of Indian adults), celiac disease, inflammatory bowel conditions, and chronic acidity medication use all impair iron absorption. You can consume 30 mg of iron daily and still absorb less than 2 mg.
Symptoms Beyond Hair Loss
Iron deficiency doesn't announce itself clearly. The symptoms are vague, overlapping with stress, thyroid issues, and busy urban life:
- Extreme fatigue: That 3 PM crash isn't just poor sleep-it's cellular oxygen deprivation
- Brittle nails: Vertical ridges, easy breakage, spoon-shaped nails (koilonychia)
- Restless leg syndrome: Uncomfortable sensations in legs, especially at night
- Pica: Craving ice, chalk, or other non-food items (yes, this is real)
- Cold sensitivity: Always needing a sweater while others are comfortable
- Cognitive fog: Difficulty concentrating, memory problems, mental fatigue
If you have three or more of these symptoms plus hair loss, iron deficiency is likely-even if your hemoglobin is "normal."
The Right Way to Test and Treat Iron Deficiency
Complete Iron Panel (Not Just Hemoglobin)
- Serum Ferritin: Target 70+ ng/mL for hair growth (not the lab's 15+ ng/mL "normal")
- Serum Iron: Should be 60-170 mcg/dL
- Total Iron Binding Capacity (TIBC): Elevated in deficiency
- Transferrin Saturation: Should be above 20%
- Complete Blood Count (CBC): Check for microcytic anemia
Supplementation Strategies That Actually Work
Oral Iron Supplementation (First-Line, But Challenging):
- Your doctor will prescribe appropriate iron supplements based on your ferritin levels
- Take with vitamin C (orange juice) to enhance absorption
- Avoid tea, coffee, dairy, and calcium supplements within 2 hours
- Common side effects include constipation-discuss alternatives with your physician if intolerable
- Requires 6-12 months to restore ferritin to optimal levels for hair growth (70+ ng/mL)
IV Iron Infusion (For Severe Deficiency or Oral Intolerance):
- Single infusion delivers high-dose iron directly to bloodstream
- Ferritin levels rise to target range within 4-6 weeks
- Hair regrowth visible within 3-4 months (faster than oral)
- Cost: ₹8,000-15,000 per infusion in Bangalore
- Requires medical supervision and is not suitable for everyone-discuss with your physician
Why Scalp Mesotherapy Works When Oral Iron Fails
Hair Mesotherapy delivers iron, biotin, amino acids, vitamins, and peptides directly into the scalp dermis - bypassing the gut entirely. For women with malabsorption, this produces results oral supplementation cannot achieve.
Protocol: 6-8 sessions spaced 2-3 weeks apart. Visible regrowth by Month 3-4. Combines perfectly with oral iron supplementation for maximum effect.
The Timeline: When Will Your Hair Stop Falling?
Understanding the hair growth cycle prevents panic during treatment:
- Month 1-2: Ferritin levels begin rising, but shedding may continue (existing follicles in telogen phase still falling out)
- Month 3-4: Shedding slows significantly as new anagen (growth) phase begins
- Month 6: Noticeable regrowth along hairline and part-baby hairs emerge
- Month 9-12: Density returns to pre-deficiency levels if ferritin maintained above 70 ng/mL
Patience is non-negotiable. Hair grows 0.5 inches per month-there are no shortcuts.
PCOS and Androgenic Hair Loss:
When Hormones Attack Your Hairline
The PCOS-Hair Loss Pathway
Polycystic Ovary Syndrome affects 10-15% of Indian women in urban areas-one of the highest global prevalence rates. The condition creates a hormonal cascade that directly targets hair follicles:
1. Insulin Resistance → Elevated Androgens: PCOS begins with insulin resistance. High insulin levels signal ovaries to produce excess androgens (testosterone, androstenedione). These androgens convert to dihydrotestosterone (DHT)-the molecule that miniaturizes hair follicles.
2. DHT Sensitivity: Indian women have higher 5-alpha reductase enzyme activity (converts testosterone to DHT) in scalp tissue. Combined with genetic sensitivity to DHT, this creates aggressive follicle miniaturization-especially at temples and crown.
3. Chronic Inflammation: PCOS causes low-grade systemic inflammation. Inflammatory cytokines disrupt the hair growth cycle, forcing follicles prematurely into telogen phase.
PCOS Prevalence in Urban India
Indian women in metro cities show 10-15% PCOS prevalence-double the 5-7% seen in Western populations. Contributing factors: sedentary lifestyles, high-glycemic diets, genetic predisposition, and chronic stress.
Of women with PCOS, 60-70% experience some degree of androgenic hair loss by age 35.
PCOS Hair Loss vs. Iron Deficiency: How to Tell the Difference
| Feature | Iron Deficiency Hair Loss | PCOS Androgenic Hair Loss |
|---|---|---|
| Pattern | Diffuse thinning across entire scalp | Male-pattern: temples, crown, widening part |
| Shedding | Extreme (200+ hairs daily) | Moderate (100-150 daily), but progressive |
| Hair Texture | Thin, brittle, breaks easily | Miniaturized (fine "vellus" hairs replace thick "terminal" hairs) |
| Other Symptoms | Fatigue, brittle nails, cold sensitivity | Irregular periods, acne, facial hair, weight gain (central obesity) |
| Blood Tests | Low ferritin (<40 ng/mL) | Elevated testosterone, LH:FSH ratio >2:1, elevated insulin |
| Reversibility | Fully reversible with iron restoration | Partially reversible with hormone control + regenerative treatments |
Important: Many women have both iron deficiency and PCOS-treating only one will produce incomplete results.
Medical Management: Controlling the Hormonal Root Cause
No topical treatment will work if androgens remain elevated. Medical management is non-negotiable:
1. Insulin Sensitizers (First-Line)
- Prescription medications: Your endocrinologist may prescribe insulin-sensitizing medications that reduce insulin resistance and lower androgen production by 20-30% within 3-6 months
- Natural supplements: Certain natural supplements (under medical guidance) may help improve ovulation and reduce androgens with minimal side effects
2. Anti-Androgen Medications
- DHT blockers: Medications that block DHT receptors in hair follicles, reduce sebum production, and slow hair loss within 3-6 months-prescribed based on your hormone profile
- Enzyme inhibitors: Some medications block the conversion of testosterone to DHT, preventing further follicle miniaturization. Requires strict pregnancy prevention protocols
- Hormonal contraceptives: Birth control pills with anti-androgenic properties regulate cycles and suppress ovarian androgen production
3. Lifestyle Modifications (As Effective as Medication)
- Low-glycemic diet: Reduce refined carbs, eliminate sugar-insulin spikes directly worsen PCOS
- Strength training: Builds insulin-sensitive muscle tissue, reduces visceral fat
- Weight loss (if overweight): 5-10% body weight reduction restores ovulation in 70% of women, lowers androgens by 15-25%
Why Medical Management Alone Isn't Enough
Even with perfect hormone control, miniaturized follicles won't spontaneously regenerate. Once DHT has damaged a follicle for months or years, it enters dormancy. This is where regenerative treatments become essential:
- Growth Factor Concentrate (GFC): Concentrated platelets deliver PDGF, VEGF, TGF-β, and EGF directly to dormant follicles, signaling them to re-enter anagen phase
- Platelet-Rich Plasma (PRP): Similar mechanism to GFC but with some red blood cells; slightly more inflammatory response
- Exosome Therapy: Cell-free regenerative signals that activate dormant stem cells without using your own blood; emerging as the most potent option
The Synergy Approach: Hormones + Regeneration
Best outcomes occur when combining anti-androgen medication (stops further damage) with regenerative treatments (awakens damaged follicles). Studies show 40-60% density improvement over 12-18 months with combination therapy versus 15-25% with either approach alone.
Protocol: Start prescribed hormone-regulating medications immediately. Begin GFC/PRP at Month 2-3 once hormones stabilize. Continue both for 12 months, then maintain with quarterly GFC sessions.
Thyroid Dysfunction:
The Hidden Saboteur of Hair Growth
Why Thyroid Disorders Cause Diffuse Hair Loss
Your thyroid gland regulates cellular metabolism-the rate at which every cell in your body consumes energy and performs its function. Hair follicle cells are metabolically hyperactive, requiring enormous thyroid hormone support to maintain their rapid division cycle.
When thyroid function drops (hypothyroidism) or spikes (hyperthyroidism), hair follicles respond quickly:
Hypothyroidism (Most Common):
- Slowed cellular metabolism forces follicles into premature telogen phase
- Reduced protein synthesis weakens hair shaft structure-hair becomes brittle
- Decreased sebum production makes scalp dry, worsening breakage
- Hair grows slower, sheds faster, and new hairs are finer
Hyperthyroidism (Less Common):
- Accelerated metabolism shortens anagen phase-hair doesn't grow as long
- Excessive shedding occurs as follicles cycle too rapidly
- Hair becomes fine, soft, and prone to breakage
The Indian Context: High Thyroid Dysfunction Prevalence
Approximately 10% of Indian women have thyroid disorders-predominantly hypothyroidism. Contributing factors include iodine deficiency (despite salt fortification), autoimmune predisposition, and genetic variants more common in South Asian populations.
The problem: thyroid disorders are often missed. Symptoms overlap with stress, anemia, and PCOS. Many women receive iron supplements and told to "manage stress" while subclinical hypothyroidism silently sabotages hair follicles for years.
Complete Thyroid Panel (Not Just TSH)
- TSH (Thyroid Stimulating Hormone): Should be 0.5-2.5 mIU/L for optimal hair growth (not the lab's 0.4-4.5 range)
- Free T4 (Thyroxine): Measures actual circulating hormone
- Free T3 (Triiodothyronine): The active form-many women have poor T4→T3 conversion
- Anti-TPO Antibodies: Detects Hashimoto's thyroiditis (autoimmune hypothyroidism)
- Anti-Thyroglobulin Antibodies: Secondary autoimmune marker
Treatment: Hormone Replacement and Optimization
Thyroid Hormone Replacement: Your endocrinologist will prescribe thyroid hormone replacement tailored to your specific lab values. It takes 6-8 weeks to normalize TSH levels, and 4-6 months for hair regrowth to become visible. Many women need TSH optimized to lower-normal range (1.0-2.0 mIU/L) for optimal hair outcomes-not just "normal" range.
Combination Therapy: Some women don't efficiently convert the standard thyroid hormone to its active form. Your physician may prescribe combination therapy to improve energy and accelerate hair recovery. This requires careful monitoring to avoid side effects.
Natural Thyroid Extracts: Some patients report better hair outcomes with natural desiccated thyroid containing multiple thyroid hormones, though dosing is less precise and requires close medical supervision.
Thyroid Hair Loss + Iron Deficiency: A Common Combination
Hypothyroidism impairs iron absorption and increases menstrual blood loss (heavier periods are common). This creates a vicious cycle: thyroid dysfunction causes iron deficiency, which worsens hair loss independently of thyroid issues.
Treatment strategy: Correct both simultaneously. Thyroid medication should be taken in the morning on an empty stomach, iron supplement in the evening with vitamin C. Space them 4+ hours apart-iron blocks thyroid medication absorption.
When to Add Regenerative Treatments
If thyroid levels normalize (TSH 1.0-2.0 mIU/L, ferritin >70 ng/mL) but hair density doesn't improve after 6-9 months, dormant follicles need reactivation. GFC therapy combined with mesotherapy delivers growth factors and nutrients directly to follicles, bypassing systemic absorption issues.
This is especially effective in long-standing hypothyroidism where follicles have been dormant for 2+ years.
GFC vs. PRP vs. Exosomes vs. Mesotherapy:
The Evidence Hierarchy for Female Hair Loss
Once you've addressed the root cause (iron, PCOS, thyroid), regenerative treatments accelerate follicle recovery and restore density. Here's what actually works, ranked by evidence quality and cost-benefit ratio:
The Complete Treatment Comparison
| Treatment | Mechanism | Evidence Level | Density Improvement | Sessions Required | Cost per Session | Best For |
|---|---|---|---|---|---|---|
| Growth Factor Concentrate (GFC) | Concentrated platelets (no RBCs) deliver pure growth factors: PDGF, VEGF, TGF-β, EGF to follicles | High (multiple RCTs) | 30-40% at 6 months | 4-6 initial, then every 6-9 months | ₹8,000-12,000 | Iron deficiency hair loss, PCOS with hormone control, diffuse thinning |
| Platelet-Rich Plasma (PRP) | Platelets + some RBCs; growth factors with mild inflammatory response | High (extensive RCTs) | 20-30% at 6 months | 6-8 initial, then every 6-9 months | ₹6,000-10,000 | Budget-conscious, early-stage hair loss, combination with mesotherapy |
| Exosome Therapy | Cell-free nanoparticles with regenerative signals; activates dormant stem cells without blood draw | Moderate (emerging data) | 35-45% at 6 months | 3-4 initial, then every 9-12 months | ₹18,000-25,000 | Poor PRP responders, severe miniaturization, patients wanting blood-free option |
| Mesotherapy | Direct scalp injections: biotin, amino acids, vitamins, peptides, iron, zinc bypass gut absorption | Moderate (multiple observational studies) | 15-25% at 6 months | 6-8 weekly, then monthly maintenance | ₹4,000-6,000 | Iron/nutritional deficiency with malabsorption, combination therapy, maintenance after GFC |
| Topical Hair Growth Medications | FDA-approved vasodilators that increase blood flow to follicles and prolong growth phase | Very High (FDA approved, decades of data) | 10-20% at 12 months | Daily application indefinitely | ₹500-800/month | Baseline therapy for all female pattern hair loss; combines with all above treatments |
| Hair Transplant (FUE) | Surgical transfer of follicles from donor area (back of scalp) to thinning areas | Very High (permanent solution) | 80-95% graft survival | 1-2 procedures | ₹40,000-1,50,000 (total) | Advanced female pattern baldness (Ludwig 3+), stable donor area, failed medical therapy |
How to Choose the Right Treatment
Treatment Selection Framework
If you have iron deficiency + diffuse thinning: Mesotherapy (6-8 sessions) + oral iron supplementation prescribed by your physician. Add GFC if no improvement by Month 6.
If you have PCOS + androgenic pattern: Start prescribed anti-androgen medications immediately. Add GFC at Month 2-3. Expect 12 months for full results.
If you have thyroid dysfunction: Optimize hormone replacement first (TSH 1.0-2.0 mIU/L). If no regrowth by Month 9, add GFC + mesotherapy.
If you have severe miniaturization (Ludwig 2-3): Consider exosome therapy for maximum follicle reactivation potential. Combine with topical medications and anti-androgens if PCOS-related.
If medical therapy + regeneratives fail after 18 months: Hair transplant consultation. Female candidates need stable donor area-diffuse thinning makes transplant challenging.
The Realistic Timeline for Results
Understanding the hair growth cycle prevents premature disappointment:
| Timeline | What's Happening | What You See | What to Do |
|---|---|---|---|
| Month 1-2 | Growth factors reach follicles; dormant stem cells activate; existing telogen hairs still shedding | Shedding may increase (normal response) | Continue treatment; resist panic; this is follicles "rebooting" |
| Month 3-4 | New anagen hairs emerge from reactivated follicles; old thin hairs are replaced by thicker ones | Fine "baby hairs" appear along hairline and part; shedding decreases | Take progress photos; maintain treatment schedule |
| Month 6 | Significant proportion of follicles in anagen phase; hair shaft diameter increases | Noticeable density improvement; ponytail feels thicker | Evaluate response; adjust treatment if suboptimal |
| Month 9 | Near-maximum follicle reactivation; hair growing longer and stronger | Visible cosmetic improvement; hairstyling easier | Discuss maintenance protocol with provider |
| Month 12 | Peak results from initial treatment protocol | 30-45% density improvement (depending on treatment modality) | Switch to maintenance: quarterly GFC or bi-monthly mesotherapy |

Hair Transplant for Women:
When to Consider, What to Expect
Why Female Hair Transplant Is Different
Male pattern baldness creates distinct bald patches with a stable "donor zone" at the back and sides of the scalp. This makes transplantation straightforward: harvest from dense area, implant in bald area.
Female pattern hair loss is typically diffuse-thinning occurs across the entire scalp, including the donor zone. This creates unique challenges:
- Limited donor hair: If the back of your scalp is also thinning, there may not be enough healthy follicles to harvest
- Unpredictable results: Transplanted follicles into a hormonally-hostile scalp (high DHT from PCOS) may miniaturize over time
- Continued native hair loss: Transplanted hair survives, but surrounding native hair continues thinning-creating a "patchy" appearance unless medical management continues
Female Hair Transplant Candidacy Criteria
You May Be a Good Candidate If:
- Ludwig Scale 2-3 with defined thinning at crown/frontal scalp
- Dense, stable donor zone at back and sides of scalp (>70 follicles/cm²)
- Failed 12+ months of medical therapy (topical medications, anti-androgens, GFC/PRP)
- Underlying cause (PCOS, thyroid) is controlled with medication
- Realistic expectations-transplant improves density 50-70%, not 100%
- Willing to continue prescribed medications post-transplant to protect native hair
FUE vs. FUT: Which Technique for Female Patients?
FUE (Follicular Unit Extraction):
- Individual follicles extracted with 0.8-1.0 mm punch tool
- No linear scar-tiny dot scars that heal invisibly
- Allows wearing hair very short (though most women prefer longer styles)
- Slightly lower graft survival (85-90%) compared to FUT
- Better for smaller sessions (1000-2000 grafts)
FUT (Follicular Unit Transplantation - Strip Method):
- Strip of scalp removed from donor area, dissected into individual grafts
- Linear scar at back of head (hidden under longer hair)
- Higher graft survival (90-95%)
- Allows larger sessions (2000-4000 grafts) in one day
- Longer recovery (10-14 days) versus FUE (5-7 days)
For most women: FUE is preferred due to no linear scar and faster recovery. FUT may be recommended for very advanced cases requiring maximum graft count.
The Transplant Timeline
- Week 1-2: Redness, scabbing at recipient site; donor area healing. Avoid exercise, no hair washing for 48 hours.
- Week 3-4: "Shock shedding"-transplanted hairs fall out (normal and expected; follicles remain intact under skin).
- Month 3-4: New growth begins emerging from transplanted follicles.
- Month 6: 40-50% of final result visible; hair still thin and growing.
- Month 12: 80-90% of final result; hair thicker, denser, mature appearance.
- Month 18: 100% final result; transplanted hair indistinguishable from native hair.
Cost and Realistic Expectations
Pricing in Bangalore: ₹40-60 per graft for FUE, ₹30-50 per graft for FUT. Most women need 1000-2500 grafts, total cost ₹40,000-1,50,000 depending on technique and clinic.
Realistic Outcomes:
- Transplant improves density by 50-70% in treated areas
- You will not have the density of your teenage years-that requires 3-4x more follicles than can be safely harvested
- Continued medical therapy (topical medications, anti-androgens) is mandatory to protect native hair
- Maintenance GFC sessions post-transplant improve graft survival and stimulate surrounding native follicles
Why Most Women Should Try GFC + Medical Therapy Before Transplant
Hair transplant is permanent, expensive, and works best when underlying causes are controlled. Since 70-80% of women with PCOS/iron deficiency/thyroid hair loss respond well to GFC + appropriate medical management, transplant should be reserved for the 20-30% who don't respond after 12-18 months of optimal treatment.
At Krity 360, we recommend GFC protocol first. If results are insufficient after 12 months, we evaluate transplant candidacy.
The 12-Month Female Hair Loss Recovery Roadmap
Here's the complete treatment roadmap based on your specific diagnosis. Every protocol starts with blood work and addressing root causes before adding regenerative treatments.
| Timeline | Iron Deficiency Protocol | PCOS Protocol | Thyroid Protocol | Combination (Multiple Causes) |
|---|---|---|---|---|
| Week 1-2 (Diagnosis) |
• Complete iron panel • CBC, ferritin, TIBC • Start iron supplementation immediately |
• Hormone panel: testosterone, LH, FSH, insulin • Pelvic ultrasound • Begin prescribed medications |
• Full thyroid panel: TSH, Free T4, Free T3, antibodies • Start thyroid medication if indicated |
• All relevant blood work • Start treating most severe deficiency first |
| Month 1 | • Iron supplementation optimized • Vitamin C with meals • Avoid tea/coffee with iron |
• Insulin-sensitizing medication initiated • Anti-androgen medication started if prescribed • Low-glycemic diet counseling |
• Thyroid medication dose adjustment based on Week 6 labs • Separate iron from thyroid meds by 4+ hours |
• Manage all conditions simultaneously • Monitor for medication interactions |
| Month 2-3 | • Recheck ferritin (target 70+ ng/mL) • Start Mesotherapy if ferritin rising but hair loss continues |
• Add topical hair growth medication if prescribed • Start GFC Session #1 • Hormones rechecked |
• TSH target 1.0-2.0 mIU/L • If optimal but hair loss continues, add GFC |
• Begin GFC + Mesotherapy combination • All underlying causes under control |
| Month 4-5 | • Mesotherapy sessions 4-6 • Oral iron continued • Expect reduced shedding |
• GFC Session #2-3 • Anti-androgen medication optimized if needed • Diet and exercise adherence reinforced |
• GFC Session #2-3 • Thyroid levels rechecked • Baby hairs emerging |
• GFC Session #2-3 • Mesotherapy biweekly • All medications optimized |
| Month 6 | • Final mesotherapy sessions • Ferritin recheck (maintain 70+) • Visible regrowth assessment |
• GFC Session #4 • Hormones normalized • 25-35% density improvement expected |
• GFC Session #4 • TSH stable • 20-30% density improvement |
• GFC Session #4-5 • Comprehensive density evaluation • 30-40% improvement if compliant |
| Month 9 | • Maintenance iron supplementation • Quarterly ferritin checks • Optional: GFC booster session |
• GFC Maintenance Session • Continue all medications • Lifestyle modifications sustained |
• GFC Maintenance Session • Thyroid levels every 6 months • Hair density near baseline |
• GFC Maintenance Session • All medical therapy continued • Near-maximum results |
| Month 12 | • Peak results achieved • Switch to maintenance: iron + quarterly mesotherapy |
• Maximum density improvement (35-45%) • Maintenance: GFC every 6-9 months + medications indefinitely |
• Final assessment • Maintenance: thyroid meds + GFC every 6-9 months |
• Complete transformation • Lifelong maintenance plan established |
Critical Success Factors
Patience: Hair grows 0.5 inches per month. Expecting visible results before Month 6 sets you up for disappointment.
Compliance: Skipping iron supplements, discontinuing prescribed medications, or missing GFC sessions guarantees suboptimal results.
Root Cause Control: Regenerative treatments (GFC, PRP, Exosomes) will fail if ferritin remains low, androgens are elevated, or thyroid is uncontrolled.
Maintenance Mindset: Female hair loss is a chronic condition. Once you achieve results, lifelong maintenance (medications, quarterly boosters) is required to sustain them.
Frequently Asked Questions: Female Hair Loss Treatment
Why do Indian women have higher rates of hair loss compared to Western countries?
Indian women face a perfect storm of contributing factors: 50-60% iron deficiency prevalence (highest globally, versus 10-15% in Western countries), predominantly vegetarian diets with poor protein and iron absorption, 10-15% PCOS prevalence in urban areas, thyroid dysfunction affecting 10% of women, chronic stress, and cultural hairstyling practices (tight buns, braids) that cause traction alopecia. Additionally, genetic variants common in South Asian populations increase sensitivity to androgens and reduce iron absorption efficiency.
How do I know if my hair loss is from iron deficiency or PCOS?
Iron deficiency causes diffuse thinning across the entire scalp, extreme shedding (200+ strands daily), brittle hair that breaks easily, fatigue, brittle nails, and cold sensitivity. Blood tests show ferritin below 40 ng/mL (though labs may call it "normal" if above 15 ng/mL).
PCOS causes male-pattern hair loss (temples and crown thinning first), moderate shedding (100-150 daily), miniaturization of hairs (thick hairs replaced by fine "vellus" hairs), facial hair growth, irregular periods, acne, and central obesity. Blood tests show elevated testosterone, LH:FSH ratio above 2:1, elevated insulin, and ovarian cysts on ultrasound.
Important: Many women have both iron deficiency and PCOS simultaneously. Comprehensive blood work is essential to identify all contributing factors.
Do iron supplements actually regrow hair, or is it just hype?
Iron supplements work only if you have iron deficiency and ferritin levels are restored to 70+ ng/mL. The challenge: most oral supplements have poor absorption (10-20%), cause constipation (leading to discontinuation), and take 6-12 months to meaningfully raise ferritin.
For women with gut absorption issues (H. pylori, celiac disease, chronic acidity medication), oral supplementation often fails. This is where Mesotherapy becomes valuable-delivering iron, biotin, amino acids, and vitamins directly to the scalp dermis, bypassing the gut entirely. Studies show visible regrowth by Month 3-4 with mesotherapy versus Month 9-12 with oral supplements alone.
Bottom line: Iron supplementation works, but only with adequate absorption and compliance. Combining oral supplementation with mesotherapy produces the best outcomes.
What's the difference between GFC, PRP, and Exosomes for hair loss?
GFC (Growth Factor Concentrate): Your blood is drawn and centrifuged to separate pure platelet concentrate without red blood cells. These concentrated platelets release growth factors (PDGF, VEGF, TGF-β, EGF) that signal dormant hair follicles to reactivate. Less inflammation than PRP, faster recovery. Evidence shows 30-40% density improvement over 6 months.
PRP (Platelet-Rich Plasma): Similar to GFC but includes some red blood cells and inflammatory markers. Slightly more post-treatment redness and discomfort. Evidence shows 20-30% density improvement over 6 months. Lower cost than GFC.
Exosomes: Cell-free nanoparticles derived from stem cells that carry regenerative signals. No blood draw required. They activate dormant stem cells in hair follicles without using your own blood. Emerging evidence shows 35-45% improvement, but costs significantly more (₹18,000-25,000 per session versus ₹8,000-12,000 for GFC).
For most women with PCOS or iron deficiency hair loss, GFC offers the best cost-benefit ratio. Exosomes are reserved for poor PRP/GFC responders or severe miniaturization cases.
How long before I see results from PRP or GFC treatment?
Hair growth follows a predictable timeline that cannot be rushed:
Month 1-2: Shedding may initially increase as dormant follicles "reboot" and enter a new growth cycle (this is normal and expected-don't panic).
Month 3-4: New hair sprouts become visible as fine "baby hairs" along the hairline and part. Shedding decreases significantly.
Month 6: Noticeable density improvement. Ponytail feels thicker. Individual hair strands are visibly thicker and stronger.
Month 9-12: Maximum results with 30-40% density increase (depending on treatment modality and underlying cause control). Hair styling becomes easier.
After Month 12, switch to maintenance protocol: GFC every 6-9 months to sustain results. Without maintenance, hair density will gradually decline over 18-24 months.
Can PCOS hair loss be reversed completely?
PCOS hair loss can be significantly improved but not always completely reversed to pre-puberty density. The degree of reversal depends on:
1. Duration of hair loss: Follicles dormant for 5+ years may not fully reactivate. Early intervention (within 2-3 years of onset) produces better outcomes.
2. Hormone control: Managing insulin resistance (prescribed medication, diet, exercise) and blocking androgens (anti-androgen medications) is non-negotiable. Without hormone control, topical treatments and regeneratives will fail.
3. Combination therapy: Best results occur when combining anti-androgen medication + GFC/PRP + topical growth medications. Studies show 40-60% density improvement over 12-18 months with this approach.
Realistic expectation: You can regain significant density and cosmetic improvement, but expecting the thick ponytail you had at age 16 may not be achievable. The goal is noticeable improvement and halting further progression.
When should I consider a hair transplant instead of PRP/GFC?
Hair transplant is considered when:
- You have advanced female pattern baldness (Ludwig Scale Grade 3) with significant crown thinning visible even with styling
- You've completed 12-18 months of optimal medical therapy (topical medications, anti-androgens, GFC/PRP) with minimal response
- You have a stable donor area-the back and sides of your scalp have dense hair (>70 follicles/cm²) that can be safely harvested
- Underlying causes (PCOS, thyroid, iron deficiency) are controlled with medication-transplanting into a hormonally-hostile scalp leads to poor results
Why most women should try GFC first: Female hair loss is typically diffuse (entire scalp thinning), making transplant challenging since the donor area may also be affected. Additionally, 70-80% of women respond well to GFC + medical management, making surgery unnecessary for the majority. Transplant works best for localized thinning (temples, frontal hairline) with a dense donor zone-less common in female patients.
How much does female hair loss treatment cost in Bangalore?
GFC (Growth Factor Concentrate): ₹8,000-12,000 per session. Need 4-6 sessions initially (spaced monthly), then maintenance every 6-9 months. Initial protocol: ₹48,000-72,000.
PRP (Platelet-Rich Plasma): ₹6,000-10,000 per session. Need 6-8 sessions initially, then maintenance every 6-9 months. Initial protocol: ₹48,000-80,000.
Exosomes: ₹18,000-25,000 per session. Need 3-4 sessions initially, then maintenance every 9-12 months. Initial protocol: ₹72,000-1,00,000.
Mesotherapy: ₹4,000-6,000 per session. Need 6-8 weekly sessions, then monthly maintenance. Initial protocol: ₹32,000-48,000.
Hair Transplant (FUE): ₹40-60 per graft. Most women need 1000-2500 grafts = ₹40,000-1,50,000 total (one-time cost).
Typical 6-month protocol: For most women with iron deficiency or PCOS, a combination of GFC (4-6 sessions) + Mesotherapy (6-8 sessions) + medications costs ₹60,000-90,000 total. This produces 30-40% density improvement in compliant patients.
Why isn't my topical hair growth medication working?
FDA-approved topical hair growth medications work by extending the growth phase and increasing blood flow to follicles. But they have limitations:
1. Doesn't address root causes: If your ferritin is 15 ng/mL, your androgens are elevated from PCOS, or your TSH is 8 mIU/L, topical medication alone cannot overcome these hormonal and nutritional obstacles. You must fix the underlying problem.
2. Requires consistent use: Skipping applications or applying only once daily (instead of the prescribed frequency) reduces efficacy by 40-50%. Most women are inconsistent.
3. Takes 6-12 months for visible results: Many women give up after 2-3 months, before the treatment has had time to work.
4. Non-responder genetics: 10-15% of women lack the enzyme needed to convert the medication to its active form. For these women, topical treatment will never work-they need alternative treatments like GFC or anti-androgens.
Solution: Combine topical medication with treatments addressing root causes (iron supplementation, anti-androgens for PCOS, thyroid medication) and add regenerative therapy (GFC) if no improvement after 6 months of consistent use.
Can stress alone cause permanent hair loss?
Stress causes telogen effluvium-acute, diffuse shedding triggered by physical or emotional shock (surgery, childbirth, severe illness, psychological trauma, crash dieting). This is temporary and fully reversible.
Timeline of stress-induced hair loss:
- Stressful event occurs (surgery, childbirth, COVID-19 infection, job loss)
- 2-3 months later, massive shedding begins (100-300 hairs daily)
- Shedding continues for 3-6 months
- Regrowth begins spontaneously as stress resolves-no treatment needed
- Full recovery by 12-18 months post-event
Chronic stress does NOT cause permanent androgenic hair loss. If you've been "stressed" for 5 years and hair continues thinning progressively (not just shedding episodes), the problem is not stress-it's PCOS, iron deficiency, thyroid dysfunction, or genetic female pattern baldness. Blaming stress delays proper diagnosis and treatment.
Do hair growth shampoos, serums, and oils actually work?
The uncomfortable truth: most topical products marketed for hair growth have minimal to no evidence of efficacy.
What doesn't work:
- Biotin shampoos (biotin doesn't penetrate scalp; must be ingested)
- Onion juice, curry leaves, fenugreek, amla oil (traditional remedies with zero clinical trials showing hair regrowth)
- "Hair growth serums" containing peptides, stem cells, or plant extracts-underdosed, poor penetration, no rigorous testing
- Caffeinated shampoos (caffeine concentration too low to have biological effect)
What has some evidence:
- FDA-approved topical medications: Only scientifically proven topical for female hair loss. Must apply as prescribed by physician.
- Prescription anti-fungal shampoos: Also have mild anti-androgen effects when prescribed by your dermatologist. Use as directed.
- Rosemary oil: One small study showed results comparable to lower-strength topical medications. Requires consistent daily application.
Bottom line: If a product costs ₹2,000+ and promises miraculous results without clinical trial data, it's marketing, not medicine. Spend that money on proper blood work and evidence-based treatments instead.
Can I do all hair loss treatments at Krity 360, or do I need multiple specialists?
At Krity 360, we provide comprehensive hair loss management under one roof:
- Complete diagnostic workup: Iron panels, hormone testing, thyroid function, nutritional assessment in association with premier labs
- Medical management: Prescription medications, iron supplementation protocols, thyroid optimization
- Regenerative treatments: GFC therapy, PRP, Exosomes, Mesotherapy
- Surgical solutions: Hair transplant (FUE/FUT) when appropriate
- Coordinated care: One treatment timeline, one medical team, no confusion about conflicting advice from multiple specialists
This integrated approach ensures that underlying causes (iron, PCOS, thyroid) are treated simultaneously with regenerative therapies for optimal outcomes. You're not shuttling between an physician, dermatologist, and hair transplant surgeon - your entire protocol is managed by one expert team.
More Articles
View All
The Executive Edge What Bangalore’s Professional Men Are Quietly Doing About Their Hair, Skin & Smile
Read Article →
The Skincare Paradox When Your Routine Is Damaging Your Skin
Read Article →